Become a Research Partners
There is currently little to no focus on JHD research. We want to empower researchers to focus on this underserved community.


What is JHD?
Huntington’s Disease is caused by an expansion of the CAG trinucleotide repeat spelling mistake (called a mutation) in the letters of DNA within the huntingtin gene. The huntingtin gene is the genetic instruction required to make huntingtin protein. Everyone has this gene and makes Huntingtin protein. However, when the DNA letters C-A-G are repeated too many times within this gene, the body makes a toxic form of the huntingtin protein. This bad version of the protein is what makes brain cells sick and ultimately leads to HD symptoms.
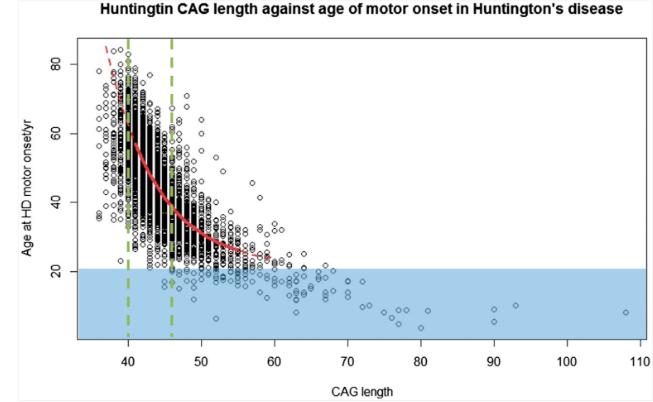
Most people who have HD have a CAG repeat of between 40-50. For these people, it is hard to tell when their symptoms will begin, as there is a lot of variability. For example, two people with the same CAG repeat of 45 could start to see symptoms of HD begin at completely different ages. But generally, a higher CAG repeat is linked to people showing HD symptoms earlier in life.
About 5% of people with HD have Juvenile HD, who tend to have higher CAG repeats, usually 50 and above, leading to their symptoms starting before their 21st birthday.
Most people (around 80%) who have JHD inherit the gene from their father. This is thought to be due to CAG repeats being less stable –meaning they can increase by larger numbers – when inherited from a male. In general, CAG repeats can increase or decrease a little when passed from generation to generation. However, in a small percentage of people there is a larger increase which can lead to JHD. It’s important to remember, however, that JHD is very rare.
Symptoms of JHD
While adult-onset HD symptoms include choreatic movement, cognitive decline and behavioral changes, JHD symptoms can vary and differ greatly due to the disease progression in a developing brain. In addition, progression of JHD is typically faster than that of adult-onset HD. However, as with adult-onset HD, there is a lot of variability in each individuals’ symptoms and how their condition progresses.
Typical early symptoms of JHD
Progression of JHD is typically faster than that of adult-onset HD. However, as with adult-onset HD, there is a lot of variability in each individuals’ symptoms and how their condition progresses.
Stiffness or Rigidity
Clumsiness
Problems with speech
Decline in Cognitive Function
Changes in Behavior
Seizures
Diagnosing JHD
Diagnosing JHD can be very difficult. As mentioned previously, JHD is rare and not many physicians have seen patients with JHD before. This can lead to a great deal of time being spent eliminating other possible causes of symptoms. Even the best physicians may need to examine a child several times before being confident of a diagnosis of JHD. A pediatric neurologist can usually determine that the child has a disorder affecting a portion of the brain called the basal ganglia (which is affected in HD) but it can be difficult to distinguish JHD from other similar diseases. It can also be difficult to be sure that early symptoms (such as changes in behavior, difficulty in school, and being clumsy) are caused by JHD. If a child shows these symptoms, it’s important to look into other causes rather than assuming it is JHD just because the condition is in the family.
Testing for JHD is not straightforward. Most young people displaying symptoms of JHD have high repeat counts which are suggestive of those symptoms being JHD. Other young people may show symptoms of JHD but don’t have high CAG repeats. The risk then is that if you test a young person for the gene the result could be in the adult-onset range. In that case, any symptoms the young person has might be due to other causes and not necessarily JHD. National and international guidelines state that unless a healthcare professional feels confident symptoms are due to JHD, a person should not be tested until they are at least 18 years old. Testing before the age of 18 takes away the person’s right to decide to be tested, and, in some countries, may cause the young person to be declined from obtaining certain benefits when they are older (such as life insurance or long-term care insurance).
Additionally, international access to clinicians who are willing and able to support families with JHD can vary greatly. As a result of all these difficulties, it can take a while for a young person to be diagnosed with JHD. There can even be people who have JHD who never receive an official diagnosis because of these challenges. This can be frustrating for everyone involved.
By collecting demographics and lived experiences, the JOIN-HD registry is hoping to achieve the following scientific goals:
Develop a database of the international JHD community who may be available and interested in participating in future research studies and trials.
Understand the prevalence and locations of the international communities.
Advocate for future research initiatives.
Use lived experiences to gather other measurable disease impacts that are important to families.
Future stages of JOIN-HD will include clinician-led interviews to further understand the family perspective.
Become A JOIN-HD Partner
These goals cannot be done by just a few people by themselves. The JHD community needs as many partners working together as possible to reach families, encourage participation, help us develop resources and much more.